
Our Electrophysiology Team strives to provide state-of-the art arrhythmia care to patients within and outside our community. Our nationally-recognized EP team’s approach can be witnessed both in the hospital and in the office.
There is no field within cardiology that has undergone as much change in the last decade than the field of electrophysiology (EP). With advances in catheter-based ablation and implantable cardiac devices, we are able to tackle (and frequently cure) diseases previously considered untreatable.
We do this in many ways. First, we keep up with national trends and the newest procedures. The board-certified physicians and staff of Oklahoma Heart Institute attend national and regional meetings to make sure we are at the cutting edge of arrhythmia management. This allows us to perform not only simple ablation such as supraventricular tachycardia (SVT) and atrial flutter, but also complex ablations including atrial fibrillation and ventricular tachycardia.
Second, we educate our local community so that they can help us identify and treat patients in the most appropriate way. Our annual EP Symposium attracts over 300 healthcare providers from throughout the region. We also host quarterly Tulsa EP Society (TEPS) meetings which are aimed at local physicians, physicians-in-training and staffs of all Tulsa’s EP community.
Third, we participate in numerous research studies. This allows our patients to access medications and devices prior to market release. Examples of research studies we offered our patients include the ATHENA Trial and the Re-Ly Trial. These trials (both published in the New England Journal of Medicine) showcased dronedarone and dabigatran – medications which will change the way we treat atrial fibrillation for years to come.
Last, we collaborate extensively with our non-EP colleagues. We understand that patients often have complex medical issues that require thoughtful discussion with a variety of specialists. Because Oklahoma Heart Institute includes many subspecialists, including cardiovascular surgeons, interventional cardiologists and heart failure specialists, we are able to join forces to streamline your care like no one else.
If you or a loved one needs to see an arrhythmia specialist, the EP Team at Oklahoma Heart Institute will provide you with the best care available. We look forward to earning your trust and having you see what sets us apart.
Heart Rhythm Service
Oklahoma Heart Institute’s Heart Rhythm Service is the largest team of electrophysiology specialists in northeast Oklahoma offering state-of-the-art arrhythmia care. They provide a full array of advanced services to patients who need help regulating their heart rhythm including evaluation, diagnosis and therapy for conditions such as atrial fibrillation, ventricular arrhythmias and devices for congestive heart failure.
Our electrophysiology team specializes in catheter ablation for a variety of heart rhythm abnormalities. Also, every year they implant hundreds of pacemakers and defibrillators with cutting edge techniques to maintain or resynchronize the heart’s normal conduction system. Each device is carefully chosen to ensure its specific features are tailored to their patient’s needs. Our Heart Rhythm Service also provides the regular monitoring and adjustments needed to ensure all devices are performing effectively. Thousands of pacemaker evaluations are performed yearly by their electrophysiologists and specialized pacing nurses.
Treatment options vary according to a patient’s health history, symptoms and preferences. Our arrhythmia specialists take these factors into account during the initial thorough evaluation.
CARDIAC RESYNCHRONIZATION THERAPY (CRT)
A CRT device is a special type of pacemaker for certain patients with heart failure. The implanted device paces both the left and right ventricles (lower chambers) of the heart at the same time. This helps to resynchronize muscle contractions and improve the efficiency of the weakened heart.
CARDIOVERSION
This is a brief procedure where an electrical shock is delivered to the heart to convert an abnormal heart rhythm back to a normal rhythm.
CATHETER ABLATION
During this procedure, flexible thin tubes (catheters) are guided into the blood vessels and to the heart muscle. A burst of energy heats to destroy very small areas of tissue that cause the abnormal electrical signals.
CRYOBALLOON ABLATION
While initial ablation procedures involved the delivery of a radiofrequency “burn” lesion at a single point, today’s cryoballoon ablation delivers a continuous circular lesion around the ostium of the vein with a single application of cryoablation. This simplified approach to pulmonary vein isolation results in a significant reduction in procedure duration and X-ray radiation exposure to the patient.
DEFIBRILLATOR
Implantable cardioverter-defibrillators (ICDs) continuously monitor the heart rhythm, automatically function as pacemakers for heart rates that are too slow and deliver life-saving shocks if a dangerously fast heart rhythm is detected. These devices are 99 percent effective in stopping life-threatening abnormal heart rhythms and are the most successful option to treat ventricular fibrillation (VF), the major cause of sudden cardiac arrest (SCA).
DEVICE EXTRACTION
In addition to implantation, Oklahoma Heart Institute’s electrophyiologists have experience with the removal of previously implanted pacemaker and defibrillator leads. At specialized centers such as Oklahoma Heart Institute, removal of pacing leads can be accomplished nearly 100 percent of the time without open heart surgery and with minimal risk to the patient.
FARAPULSE Pulsed Field Ablation System
LEFT ATRIAL APPENDAGE CLOSURE (LAA)
It is estimated that 90 percent of heart clots that cause strokes come from the left atrial appendage closure (LAA). By closing off the LAA, the risk of stroke may be reduced and over time, patients may be able to stop taking warfarin. The highly successful implant offered to help close off the LAA:
WATCHMAN FLX™ DEVICE IMPLANT
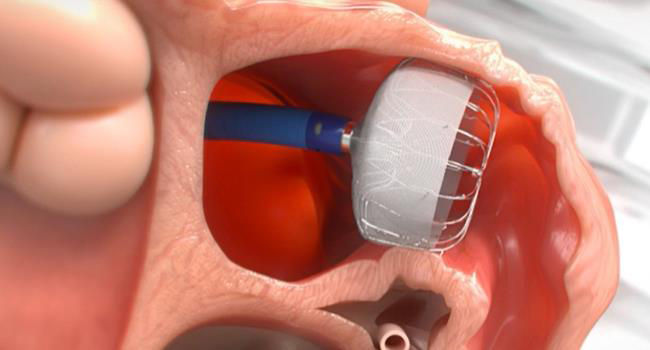
This device offers a stroke risk reduction option for high-risk patients with non-valvular atrial fibrillation who are seeking an alternative to long-term warfarin therapy. This minimally invasive procedure usually takes one to two hours and is done under anesthesia. Usually this is a one-time procedure that offers significantly less pain than with open heart surgery. Most patients are normally able to stop taking their blood thinners around 45 days post-procedure.
MEDICATION
People with atrial fibrillation (AFib) are five times more likely to have a stroke than people without AFib. Stroke reduction therapy is usually directed at thinning the blood with anticoagulants (blood thinners). While blood thinners have been shown to significantly improve survival, it is important to assess each patient’s benefit to risk ratio.
Anticoagulants
- Traditional: Warfarin (Coumadin & Jantoven)
- Novel Oral Anticoagulation (NOAC)/Direct Oral Anticoagulant (DOAC): Apixaban (Eliquis), Dabigatran (Pradaxa), Edoxaban (Savaysa) and Rivaroxaban (Xarelto)
If appropriate, antiarrhythmic medications can be used to help manage arrhythmias. They are sometimes used as a first line therapy prior to undergoing an ablation procedure.
Antiarrhythmic Medications
- Amiodarone (Cordarone & Pacerone)
- Dofetilide (Tikosyn)
- Dronedarone (Multaq)
- Flecainide (Tambocor)
- Propafenone (Rythmol & Rythmol SR)
- Sotalol (Betapace & Betapace AF)
PACEMAKER
A pacemaker is a small, battery-operated device that helps control an abnormal heart rhythm which is sometimes called arrhythmia or dysrhythmia. Some pacemakers are permanent (internal) and are implanted under the skin of the chest or abdomen while others are temporary (external). This device uses electrical pulses to “pace” the heart or prompt it to beat at a normal rate which can relieve common symptoms such as fatigue and fainting. Most pacemakers are designed to detect the amount of activity a patient is doing and adjust the heart rate appropriately.
Oklahoma Heart Institute was the first center in northeast Oklahoma to offer a better pacemaker technique called his-bundle pacing. Traditionally, pacemaker wires are placed in the muscle at the bottom of the heart which leads to a more forced heart squeeze. This can sometimes cause weakening of the heart muscle (cardiomyopathy) over time and eventually congestive heart failure. His-bundle pacing places the pacemaker wires very close to the actual conduction system (nerves in the heart) for a more normal and natural heart squeeze.
RISK FACTOR MODIFICATION
Since other heart disorders increase the risk of developing abnormal heart rhythms, lifestyle changes often are recommended. Living a heart healthy lifestyle can ease the symptoms experienced with heart rhythm disorders and other heart disorders and can be beneficial to overall patient health.
While genetics and age play a significant role in atrial fibrillation (AFib), there are modifiable risk factors which can dramatically improve symptoms and frequency of this arrhythmia. Modifiable risk factors include weight, sleep apnea, alcohol consumption, tobacco usage, blood pressure control and diabetic management. Controlling these risk factors can drastically improve the ability to treat and prevent AFib.
Contact Us
For more information or to schedule an appointment, please call 918-592-0999.
Heart Rhythm Service Providers
Click on a Provider to View More Information








