
The Advanced Heart Failure Center
The Advanced Heart Failure Center at Oklahoma Heart Institute (OHI) is a recognized Get With The Guidelines® Heart Failure center that provides comprehensive cardiac care to patients with advanced heart failure and pulmonary hypertension. We specialize in the evaluation and implementation of treatment plans for patients with complex cardiovascular disease with the goal of cardiac recovery. In those patients who experience progression of disease and are eligible, we provide an array of advanced therapies including continuous home infusions, implantation of durable left ventricular assist devices (LVADs), timely referral to a transplant center and access to greater support at home in the form of palliative or hospice care.
Our center utilizes a comprehensive multidisciplinary approach for the care of our patients. We work closely with various medical and surgical specialties and subspecialties available at OHI to manage our patients. We are a key step in the evaluation and referral process to a variety of FDA-approved percutaneous valvular replacement interventions performed by our highly trained structural cardiology team (TAVR, Mitra-clip, Mitral II trial, CLASP IIF trial, TRISCEND II trial). We have also expanded the therapeutic armamentarium available to advanced heart failure patients to include devices that seek to improve patient’s symptoms, like the Barostim device, or treat a once untreatable condition in patients with reduced ejection fraction, such as central sleep apnea with the remedē® System.
We are the only center in Tulsa supported by an extracorporeal membrane oxygenation (ECMO) program, which allows us to support and bridge many of our patients safely to recovery or to the implantation of a durable heart pump (left ventricular assist device) or heart transplant. Our team of highly trained cardiologists, intensivists, surgeons, advanced practice providers, specialized nurses, cardiac care coordinators, social workers, case managers, therapists, exercise physiologists and other experts are at the disposition of our patients to improve their symptoms, quality of life and survival.
For patients
The patient is our top priority at the Advanced Heart Failure Center. We will provide the education and tools needed to understand the diagnosis of heart failure or pulmonary hypertension, and the treatment options available to you.
What to expect at the first appointment:
We ask that you arrive 15 minutes early to fill out the necessary paperwork and to bring all medication bottles with you. After meeting with the provider, one of our nurses will meet with you to provide heart failure education. We also provide you with a blood pressure cuff, weight scale and water bottle to help with the daily management of your heart condition.
What to expect at each appointment:
Please bring your medication bottles and daily weight/blood pressure log with you to every appointment. Each time, we will take your weight and vital signs.
Our clinic has a nurse on-call 24/7 for emergencies. Our goal is to manage your care outpatient and keep you out of the hospital.
For providers
Our team of physicians, advanced providers and nurses specialize in the diagnosis and treatment of advanced heart failure and pulmonary hypertension. The clinic is located within the OHI hospital, on the campus of Hillcrest Medical Center, which allows us to provide a comprehensive fluid management program, including evaluation and treatment with intravenous diuresis, hydration and electrolyte replacement in the outpatient setting. We can obtain electrocardiograms, telemetry monitoring and collection of labs with same-day results. Rapid assessment of the efficacy of outpatient therapies facilitates the decision to discharge home versus direct-admit to the hospital for further escalation of care. The clinic has a nurse on-call 24/7 for emergencies. Our highly specialized registered nurses provide every new patient consult with heart failure education and continued re-enforcement. Our goal is to reduce hospital readmissions and improve patients’ quality of life.
Please keep in mind an early referral is essential in those patients whom we suspect are progressing into advanced heart failure and require an evaluation for advanced therapies, including transplant or LVAD evaluation. We believe in a shared care model within our practice and encourage patients to continue their follow-up visits with those referring physicians who would like to remain involved in the management of their patients’ care.
Please see below for the wide range of services we provide here in the Advanced Heart Failure Center. We look forward to partnering with you.
Extracorporeal Membrane Oxygenation (ECMO) is for patients who are extremely sick due to acute heart and/or lung failure that is potentially reversible and unresponsive to conventional management. The ECMO machine helps to alleviate the stress on these vital organs in order for them to have a chance to rest and recover until they are able to properly function again. Placing a patient on ECMO is done either in the operating room, cath lab or at the patient’s bedside. When connected to an ECMO machine, the blood flows through a tube into an artificial lung for the purpose of removing carbon dioxide and adding oxygen. Then, the blood is warmed to body temperature and pumped back into the body. Depending on the condition of the patient, they may stay on ECMO anywhere from just days to several weeks. During this time, the medical team is able to treat them with a variety of procedures, medicines or give them adequate time to recover.
ECMO is used:
- To assist patients recovering from heart failure, lung failure or heart surgery
- During an LVAD (left ventricular assist device) procedure or similar
- During high-risk cardiac catheterization lab procedures
- Overwhelming infection
- Burn injury to the lungs
- Acute heart failure
- Blood clot in the lungs
- Low body temperature
- Drug intoxication
- Chest trauma
- Influenza
- Pneumonia
ECMO Referrals
For urgent inpatient referrals, please call 1-833-OHI-ECMO (644-3266)
The LVAD is an implantable mechanical pump that supports a weak left ventricle and helps pump blood to the rest of the body. This mechanical circulatory support device can be a therapy option for symptomatic patients with advanced heart disease that centers around a weak left ventricle.
OHI is the only hospital in northeast Oklahoma that offers this advanced therapy with the implantation of the HeartMate 3™ LVAD as a bridge to transplant or destination therapy for eligible patients. The HeartMate 3 ™ is a centrifugal flow pump that utilizes Full MagLev™ Flow technology, which helps protect the blood as it flows through the pump.
Our team includes LVAD coordinators, whose sole job is to educate and guide not only the patient, but their loved ones through the evaluation process into the pre-operative, post-operative and the long-term course afforded to patients by this durable mechanical support.
For patients
Over 6.2 million adults in the United States have heart failure. It is a complex, progressive disease associated with poor prognosis and significantly reduced quality of life, leading to increased risk of death. More than 250,000 patients are in the advanced stage of heart failure and are not eligible for a heart transplant due to their comorbidities or health histories. LVAD therapy has been demonstrated to extend life and improve quality of life for patients who may not derive any further benefit from earlier stage therapy options.
The HeartMate 3™ LVAD consists of an external system controller that monitors the pump, a modular driveline that connects the pump and controller and a battery-powered source that runs the pump and controller.
The HeartMate 3™ pump fits in the area around the heart known as the pericardial space. The pump is connected directly to the heart at the bottom of the left ventricle. There, the left ventricle draws the oxygenated blood through the pump and pushes it into the aorta where the blood flows to the rest of the body.
If you have any questions about this support system, please contact our center for more information.
For providers
If your patient experiences any of the following high-risk clinical triggers, refer them to our Advanced Heart Failure Center at OHI for an evaluation by one of our heart failure specialists for consideration of advanced heart failure therapies, including LVAD therapy.
You can quickly screen your patient using the I-NEED-HELP acronym:
I – IV inotropes
N – NYHA IIIB/IV or persistently elevated natriuretic peptides
E – End-organ dysfunction (Cr > 1.8 mg/dL or BUN > 43mg/dL)
E – EF ≤ 35%
D – Defibrillator shocks
H – Hospitalizations > 1 with heart failure
E – Edema (or elevated PA pressure) despite escalating diuretics
L – Low blood pressure, high heart rate
P – Prognostic medication – progressive intolerance or down-titration of GDMT (guideline-directed medical therapy)
Pulmonary hypertension is a life-threatening condition where the arteries between the heart and lungs are either narrowed or blocked. Treatments are available that can help reverse or prevent the progression of heart failure, and improve quality of life.
Pulmonary hypertension can be a daunting and confusing diagnosis. Pulmonary hypertension refers to increased resistance in the pulmonary vasculature that eventually leads to right-sided heart dysfunction. This commonly leads to worsening shortness of breath and/or difficulty with daily activities. Due to the subtle signs and symptoms, patients often experience a delay in their diagnosis and treatment initiation. There are many reasons for pulmonary hypertension, each requiring careful diagnosis and individualized treatment approaches.
At OHI, we specialize in diagnosis and treatment of pulmonary hypertension, which includes both medication and non-medicated approaches. We offer cardiac MRI, cardiopulmonary exercise testing and right heart catheterization to help tailor your individual plan. We are happy to develop a treatment plan to fit your lifestyle and restore your quality of life.
For providers
The Advanced Heart Failure Center at OHI accepts referrals for the evaluation, diagnosis and treatment of patients with suspected or confirmed pulmonary hypertension. We are a comprehensive care center with expertise in echocardiography, cardiac MRI, right heart catheterization with vasodilator study and both invasive and non-invasive cardiopulmonary exercise testing. These tests are critical to diagnosing and identifying the proper treatment for pulmonary hypertension patients as well as for assessing treatment response.
Our staff includes two dedicated pulmonary hypertension coordinators who help collection of medical records prior to consultation, meet with the patient to discuss the treatment plan and ensure access to therapy.
For providers
We offer the expertise in the evaluation, diagnosis and treatment of infiltrative cardiomyopathies, including cardiac amyloidosis. We evaluate patients suspected of having infiltrative cardiomyopathies with a complete array of cardiac imaging tools including transthoracic echocardiography with global longitudinal strain (GLS), cardiac MRI with late gadolinium enhancement (LGE), and technetium Tc-99m pyrophosphate (PYP) scan. Ultimately, in the case of indeterminate findings, we can proceed with invasive cardiac measures, including endomyocardial biopsy if appropriate. Our staff includes a cardiac amyloidosis coordinator that will arrange the collection of patients’ medical records prior to a consult visit, meet with the patient to discuss the treatment plan delineated by the provider, facilitate the insurance approval process of ATTR amyloidosis specific drug therapies, along with monitoring the response to treatment and follow-up cardiac studies.
In the case an AL amyloidosis diagnosis is made, we work closely with our colleagues from the oncology and hematology group at Utica Park Clinic to determine treatment or to vet any overlapping features consistent with monoclonal gammopathy of undetermined significance (MGUS).
For patients
The Advanced Heart Failure Center at OHI offers the expertise in the evaluation, diagnosis, and treatment of infiltrative cardiomyopathies, including cardiac amyloidosis (am-uh-loi-DO-sis).
Cardiac amyloidosis is a rare disease that occurs when either bone marrow or liver produces an abnormal protein called amyloid. This protein can cause problems as it builds up in various organs and soft tissues, including the heart, liver, kidneys, spleen, digestive tract, and nervous system.
There are different types of amyloidosis and symptoms can vary, depending on the affected organ or soft tissue. Amyloidosis is not curable, but its progression can be interrupted and, at times, reversed with specific therapies.
Common types of amyloidosis:
AL amyloidosis (Light Chain): The most common type of Amyloidosis, caused by a bone marrow disorder. It is often treated with chemotherapy or stem cell transplant. We work closely with our hematology/oncology colleagues, who determine the best treatment plan for these patients.
Hereditary amyloidosis (hATTR): Caused by a gene mutation and involves an amyloid protein produced in the liver. There are specific therapies that stabilize this protein or halt its production, preventing further damage and progression of the disease. These infusions and injections can be prescribed and administered in our center.
Wild-type ATTR amyloidosis: Caused by deposition of an otherwise normal amyloid protein over time, related to aging. This type can ultimately lead to heart failure. An oral regimen is the most common treatment.
Common signs and symptoms:
- Bilateral carpal tunnel syndrome
- Chronic gastrointestinal issues such as diarrhea
- Bicep tendon rupture
- Dizziness
- Fatigue
- Heart failure symptoms, such as shortness of breath and swelling in hands, arms, legs and feet
- Muscle weakness
Amyloidosis screening and diagnosis
Diagnosis can be a lengthy process. Symptoms vary and affect people differently. That is why it is important to see a doctor who has experience diagnosing and treating amyloidosis. Your signs and symptoms will determine what tests are ordered for you.
- Autonomic testing, including functions like heart rate, body temperature, breathing rate and digestion
- Biopsy of the skin, nerves, muscle, heart, liver or abdominal fat pad, the examination of a sample of tissue under a microscope
- Blood tests including genetic testing
- Cardiac MRI
- Echocardiography - an ultrasound of the heart
- Technetium Tc-99m pyrophosphate (PYP) scan of the heart
For patients
OHI performed one of the first procedures in Tulsa using the CardioMEMS™ HF System, a miniaturized, wireless monitoring sensor to manage heart failure. CardioMEMS™ is the first and only FDA-approved heart failure monitoring device that has been proven to significantly reduce hospital admissions when used by physicians to manage heart failure.
The pulmonary artery carries blood from your heart to the lungs. If your heart is too weak or stiff to pump effectively, fluid builds up and causes pressure to increase in both the heart and lungs. The CardioMEMS™ PA sensor detects these changes in pulmonary arterial pressures and allows your doctor to detect worsening heart failure often before you do.
The CardioMEMS™ HF System includes a tiny pressure-sensing device inserted into the pulmonary artery. You will also have a home unit which is about the size of a queen-size pillow that allows PA pressure readings to be sent directly to a secure website your clinician can access on a regular basis.
Every day, you lie down on the provided home unit which is approximately the size of a queen size pillow and press the start button. A reading takes only a few minutes each day, and there is no pain or sensation during the readings.
By regularly monitoring CardioMEMS™, your provider will recommend lifestyle and medication changes earlier. Being proactive helps keep you feeling better without the need for additional clinic visits and reduces the chance of hospitalization due to heart failure.
For Providers
OHI performed one of the first procedures in Tulsa using the CardioMEMS™ HF System, a miniaturized, wireless monitoring sensor to manage heart failure. CardioMEMS™ is the first and only FDA-approved heart failure monitoring device that has been proven to significantly reduce hospital admissions when used by physicians to manage heart failure.
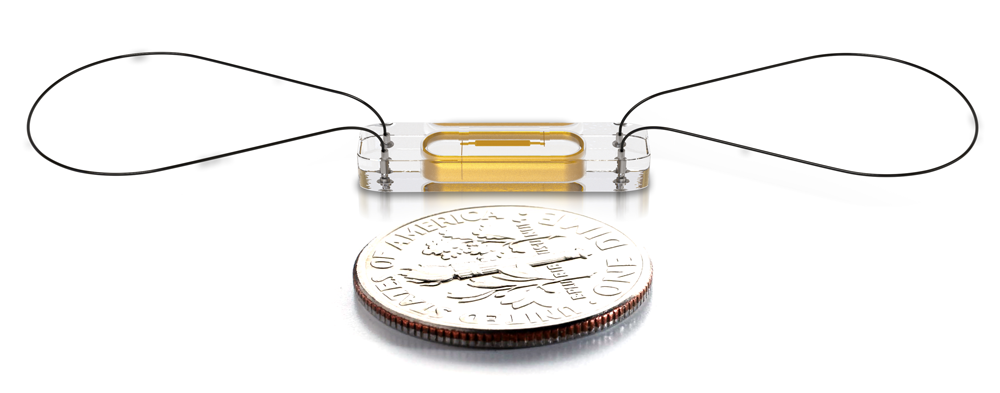 Photo courtesy of Abbott
Photo courtesy of AbbottCardioMEMS™ features a sensor that is implanted in the pulmonary artery (PA) during a right heart catheterization to directly measure PA pressure. Increased PA pressures appear before weight and blood pressure changes, which are often used as indirect measures of worsening heart failure.
The CardioMEMS™ sensor is designed to last the lifetime of the patient and does not require batteries. There is no pain or sensation for the patient during the readings. Once implanted, the wireless sensor transmits daily PA pressure readings, PA waveforms and heart rate through the patient’s home unit to a secure website, where the data is consistently reviewed by a clinician.
CardioMEMS™ allows providers with the ability to detect worsening heart failure sooner and adjust treatment to reduce the likelihood that the patient will be hospitalized.
For patients
As a part of your treatment, your doctor and health care providers may consider aquapheresis, also known as ultrafiltration therapy. This therapy safely and effectively removes excess salt and water from patients who are suffering from fluid overload due to heart failure.
Your health care provider may prescribe a low-salt diet, fluid restriction or other therapies to help reduce fluid – such as a water pill or diuretic, given orally or intravenously. However, these treatments do not always work effectively, resulting in a need for alternative therapy – such as aquapheresis.
For providers
Aquapheresis (ultrafiltration) is a process of fluid removal when a patient is diuretic resistant. A patient is considered diuretic resistant when:
- Patient is > 10 pounds over dry weight
- Previous hospitalizations with ineffective diuretic effect
- Patient cannot achieve a goal of -2 liters at 24 hours
- No significant difference in patient’s global assessment of symptoms in 24 hours.
Goals of aqupaheresis:
- Reduction in hospital readmission: prevent patients from being discharged when they are “wet” (volume overloaded)
- Reduction of length of stay if aqupheresis is started early (< 24 hours of admission)
- Stable renal function
Monitor BMP/CMP prior to starting aqupheresis can reduce rate of fluid removal as needed. This is usually managed by Advanced Heart Failure team in units with specially trained nursing staff (2 heart and 3 heart)
ALT-FLOW II Clinical Trial
Contact Us
For more information about The Advanced Heart Failure Center, please call 918-574-9003.
Referral Information
For urgent inpatient referrals, please call 1-833-OHI-ECMO (644-3266)
For non-urgent outpatient referrals, please call 1-833-OHI-LVAD (644-5823)






